Roll no. - 56
ADM NO - 176046
I HAVE BEEN POSTED IN GENERAL MEDICINE FROM 12/12/2022 TO 11/02/2023
IN THIS BLOG I'M SHARING MY INTERSHIP WORK EXPERIENCE
MY MEDICINE INTERNSHIP DUTY STARTED AND ENDED WITH UNIT POSTINGS. I WAS POSTED IN UNIT II FOR THE FIRST AND LAST 15 DAYS OF MY MEDICINE INTERNSHIP DUTIES.
These are some of the things i learnt during my unit duties :-
I did Vitals monitoring of op patients
learnt how to take history of patients coming to op
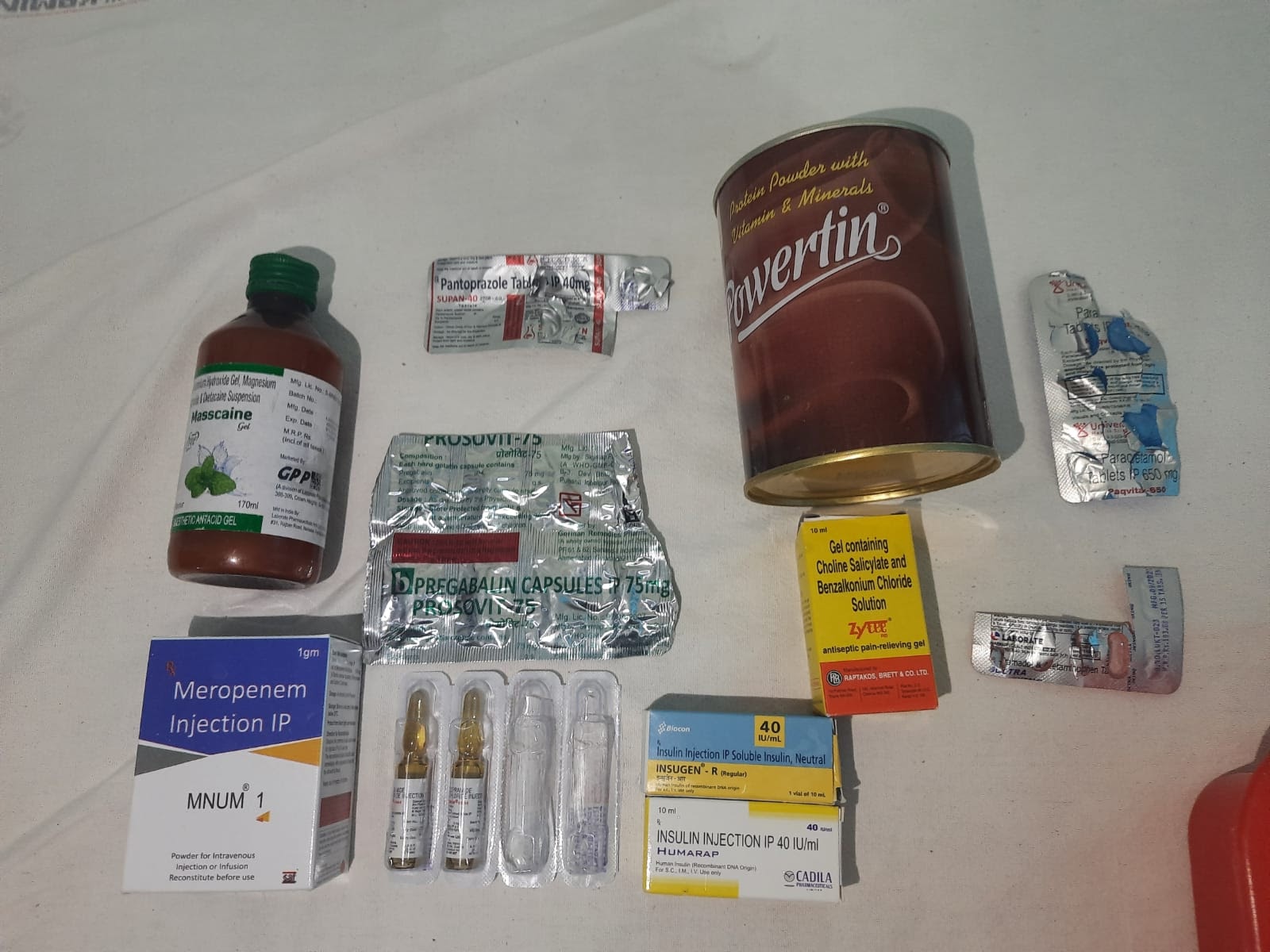
learnt prescription writing for op patients and need for each medicine prescribed
leant how to evaluate/examine patient clinically based on history
Learnt how to manage cases in casualty
learnt IV cannula insertion
learnt Ryles tube insertion
learnt how to put foleys catheter
Assisted in CPR in casualty
Learnt how to use Bains circuit and ambu bag
Drew ABG samples and venous blood samples for investigations
collected investigations reports from labs
Written repeats and investigations in case sheets, did tpr charting and updated soap notes
Learnt and typed discharge of many patients
Few of my e-log documentation of patient's clinical data is shared here :-
CASE:1
A 77 year old male with fever, cough and abdominal discomfort
My learning points from this patient's case are:
1-The types of seizures:
- Focal seizure
- Generalized seizure
Focal seizure are of 2 types:
- With impaired awareness
- Without impaired awareness
Types of Generalized seizures:
- Absence seizures
- Tonic seizures
- Atonic seizures
- Clonic seizures
- Myoclonic seizures
- Tonic clinic seizures
2- Hypoglycemia and seizures
In addition to arrhythmias, severe hypoglycemia can cause seizures, and increased frequency of seizures has been associated with mortality .In previous severe hypoglycemic clamp studies, seizures were associated with both respiratory depression and premature ventricular contractions
3- What are the most common type of seizure with hypoglycemia?
Hypoglycaemia, common in diabetic patients treated with insulin, can induce various neurological disturbances. Of these, seizures are the most common acute symptom, mainly of the generalised tonic-clonic type, with focal events.

CASE-2
My learning points from this patient's case are
1 - learnt to diagnose DKA with clinical features and investigations
2 - learnt to diagnose old Myocardial infarction
3 - learnt to diagnose diabetic nephropathy clinically
4 - learnt to manage DKA case
CASE-3
My learning points from this patient's case are
1 - learnt to manage pyrexia case
2 - learnt to manage hyponatremia
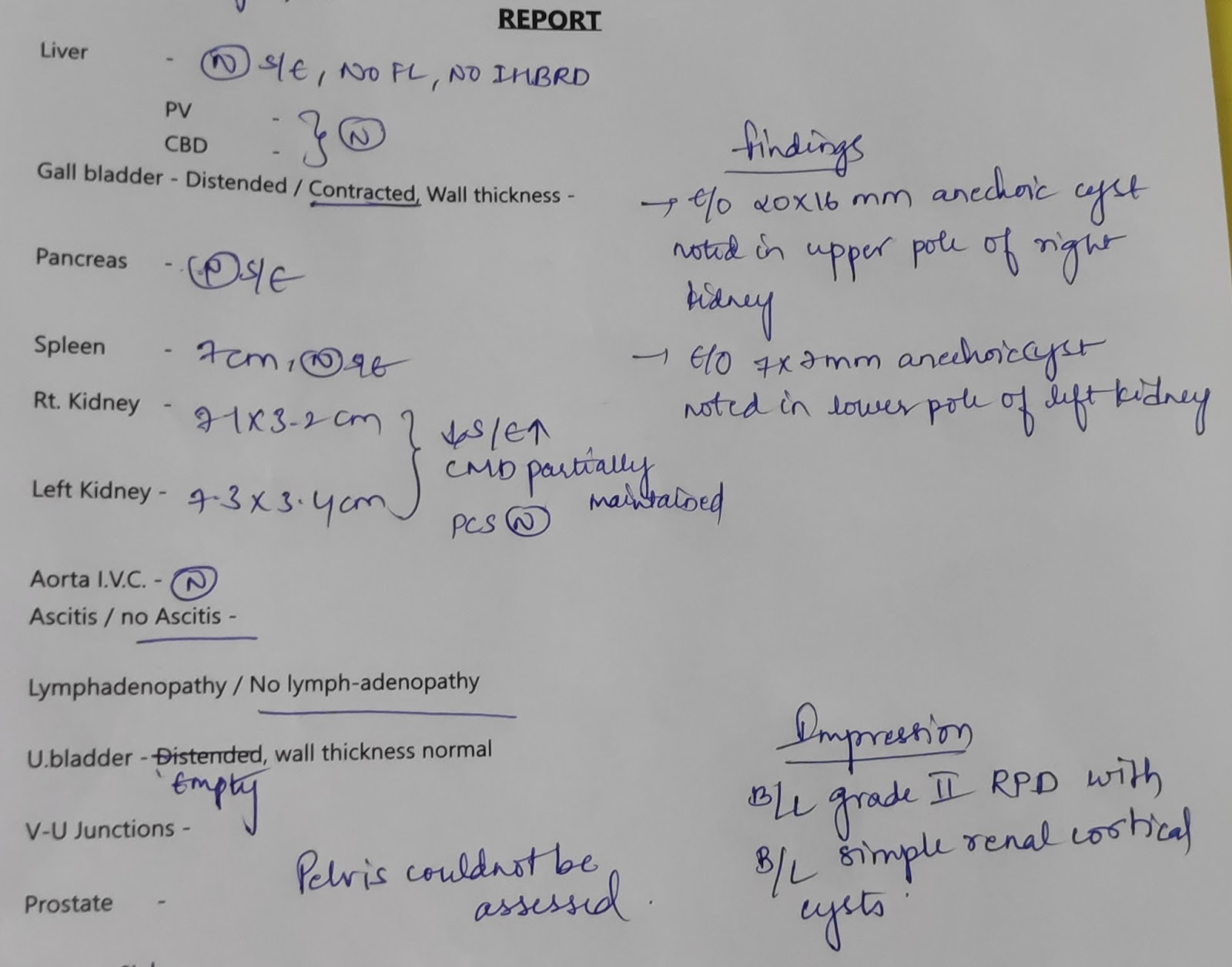
3 - learnt to diagnose ckd case
4 - learnt blood transfusion
CASE-4
1 - learnt to manage copd case
2 - learnt about ct scan
3 - learnt to use cpap


PSYCHIATRY DUTIES
I WAS POSTED IN PSYCHIATRY DEPARTMENT FOR 15 DAYS
MY LEARNING POINTS IN PSYCHIATRY POSTING:
LEART HOW TO TAKE HISTORY FOR PSYCHIATRY PATIENTS
CASES I HAVE SEEN ARE
1.ALCOHOL DEPENDENCE SYNDROME
2.ADJUSTMENT DISORDERS
3..TOBACCO DEPENDENCE SYNDROME
4.SCHIZOPHRENIA
5. OBSESSIVE COMPULSION DISORDER
learnt how to manage patients in de-addiction centre
Collected investigation reports
Did vitals monitoring of psychiatry patients
learnt how to write case sheet in psychiatry department
Learnt about various psychiatric drugs
PERIPHERALS DUTIES FOR A TOTAL 15 DAYS
WARD DUTIES 5 DAYS
Attended rounds
updated soap notes of ward patients
participated in conducting a CME
ICU DUTIES 5 DAYS
vitals monitoring for patients
Drew ABG and venous blood samples
Sent investigations
Learnt how to manage critically ill patient's
Assisted in CPR
NEPHROLOGY DUTIES 5 DAYS
Vitals monitoring for patients on hemodialysis
learns managemnet of elevated BP during dialysis.
Learnt management of ckd patients
Did ascitic fluid tapping (Abdominal paracentesis)
























































{kind=link}