This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box"
DR JATIN SHARMA
Roll no. 56
A 70yr old male agriculturer brought to casualty with
C/o dry cough since 4 days
C/o breathlessness since 4 days
HOPI :
A 70 yr. Old male agriculturer brought to casualty with complaints of dry cough since 4 days, insidious in onset, more during night then daytime, not associated with Sputum, blood tinge, chest pain. H/o seasonal variations present. Not associated with positional variation. Aggravated with fever (if present) and cold (if present). Relieved with medication.
H/o breathlessness since 4 days, upon walking to some distance(100-200mt.) mmrc grade 2-3, gradually progressive, insidious in onset, more at night compared to day, no seasonal variation since 3 yrs. diurnal variation present, no positional variation. Aggravated on exertion, relieved at rest, orthopnea present, postural nocturnal dyspnea present since 3 yrs.
Past history :
H/o similar complaints in past started from 15yrs.
Dry cough + breathlessness was present, occasionally having seasonal (winters) + diurnal (night >day) variation since 3 yrs.
His breathlessness showed no seasonal variation.
H/o RTA 20 yrs ago, which has lead to deformity in spine ( thoracic scoliosis)
H/o similar complaints in dec, 21 2d echo showed LV hypokinesia, RWMA +, EF - 48%
K/c/o HTN since 1 yr.
No H/o Dm , asthma , TB, epilepsy
Personal history :
Appetite - normal
Diet - mixed
Sleep - normal
Bowel and bladder movements - normal
Addictions - 1.previously occasional beer drinker, stopped 3 months ago
2. Started smoking beedi/chutta since 17yrs of age stopped 5days ago.
General examination :
Patient is conscious, coherent and cooperative, moderately built and moderately nourished.
Pallor: absent
Icterus: absent
Cyanosis: absent
Clubbing: absent
Lymphadenopathy: absent
Pedal edema: absent
Vitals:
BP-140/90mmhg
PR- 80
RR- 37bpm
SpO2- 95% on RA in sitting position
100% on supine
GRBS-173mg/dl
Systemic Examination :
CVS- S1S2 ; no murmur heard
RS- BLAE; diffuse ronchi heard
P/A- soft non tender
CNS- HMF intact
Clinical images :





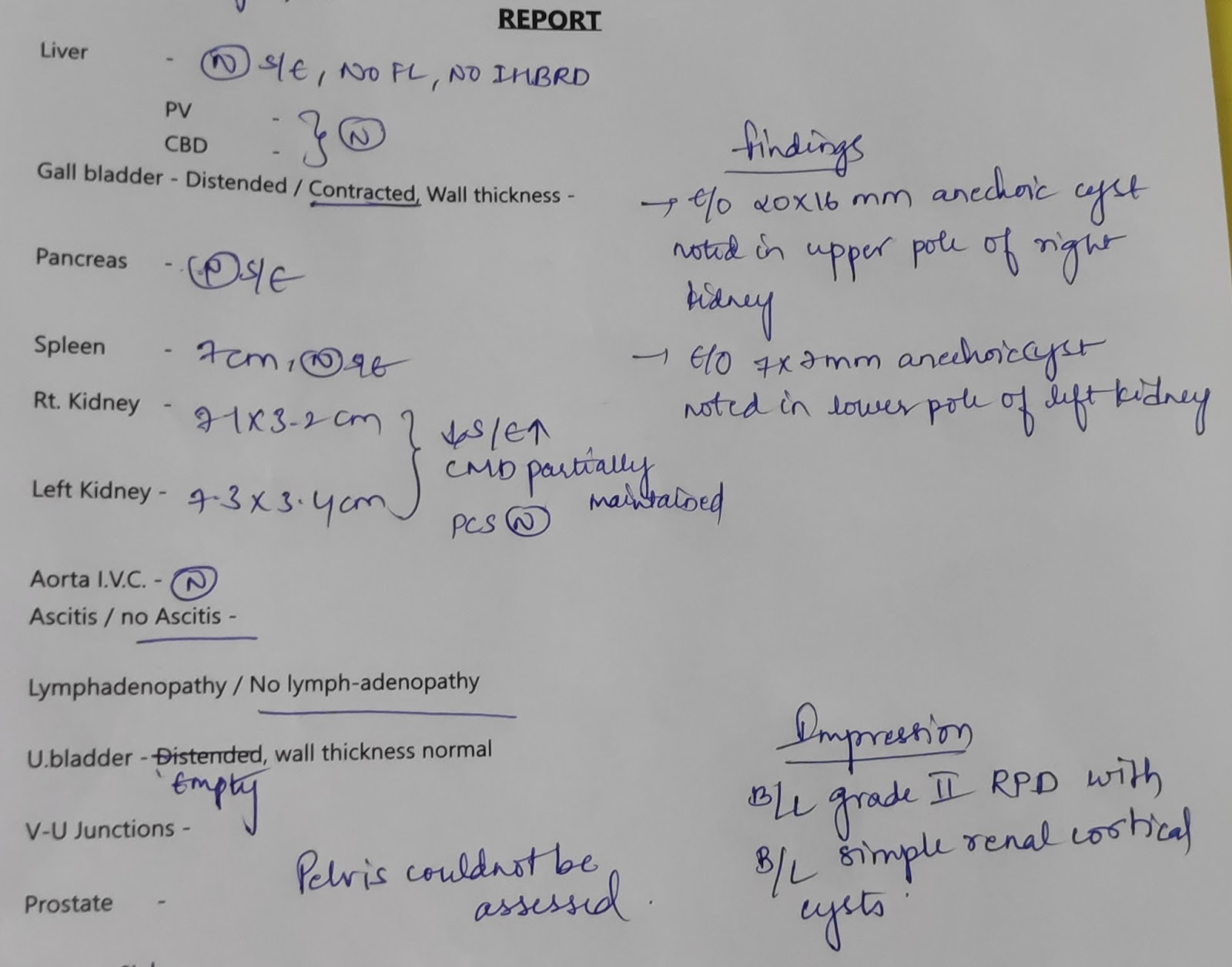
Investigations :

Chest xray PA view 25-12-22

Chest xray lateral view 25-12-22

Ecg 25-12-22


Investigations chart
Provisional Diagnosis ?COPD - Chronic bronchitis with old MI with Bi fascicular block with k/c/o HTN since 1 yr.
Treatment :
* Inj. Hydrocort 100mg iv stat
* NEB 2 respules duolin, budecort, mucomist every 6th hourly
* inj. Pan 40 mg iv od
* inj. Optineuron 1 amp. In 100 ml NS iv over 30min.
* o2 inhalation @ 2-4 L/min. ( target spo2 - 92%)
* inj. Hydrocort 100mg iv bd
* T. ASPIRIN(GASTRO-RESISTANT) 75mg
T. CLOPIDOGRIEL 75mg
T. ATORVOSTATIN 20mg
* T. Amlong 5mg po od
* monitor vitals



No comments:
Post a Comment